
Jonathan Tan, Senior Physiotherapist at Lifecare Point Walter.
In the early stages of my physiotherapy career, one of the conditions I seemed to have more difficulty managing was buttock pain, specifically a proximal hamstring tendinopathy.
A typical patient would walk in complaining of both a figurative and physical ‘pain in the butt’ when running, walking and often just sitting.
They were typically a middle-aged runner, trying to increase their training load in preparation for some of running event like the HBF Run for a Reason.
They would complain of a dull aching pain just below their buttock when warming up which would subside during the mid-portion of their run, begin to aggravate towards the end before coming on stronger than Michael Jordan in game 6 a couple of hours later.
One probable reason for our poor track record with this condition is that telling a runner to stop running is like telling a smoker to just stop smoking – running is addictive!
Then comes the question, how much can they still do?
However, after explaining the pathology behind the problem and the requirement to alter running load we can usually come to some sort of compromise.
Over the past year I’ve had some better (far from amazing) results with slight adjustments to my own approach and following evidence-based management, which I thought I’d share.
Firstly, we need to confirm that there actually is a hamstring tendinopathy and exclude other causes of buttock pain (i.e. lumbar spine referral, hip joint pain, neural structures).
Once we have our diagnosis, we can get going.

TYPICAL CLINICAL PRESENTATION OF PATIENTS WITH HAMSTRING TENDINOPATHY
- Pain after exercise and the following morning
- Often pain free at rest and initially causing pain in upper thigh/buttock with activity
- Buttock pain improves following warm-up
- Can often still complete a full training session in the early stages
- Local tenderness of the proximal hamstring tendon affected (semitendinosus, semimembranosus, biceps femoris)
- Commonly aggravated by running, walking (worse on incline) and prolonged sitting
WHAT IS A TENDINOPATHY?
We could discuss this for hours, so I’ll keep this short and simplified for you the patient’s perspective.
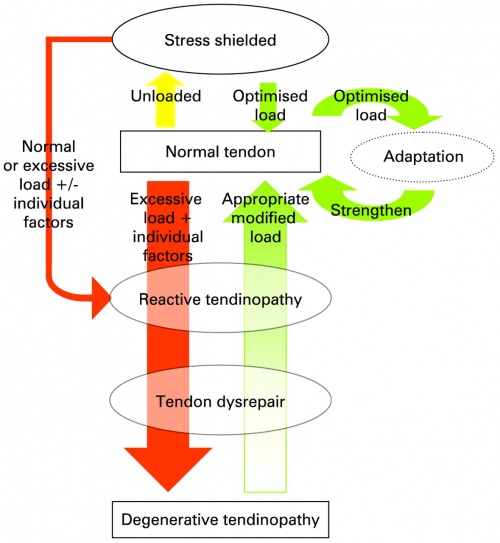
Cook and Purdam (2009)
Cook et al (2009) describes the pathology of a tendinopathy as a continuum.
Every day we load our tendons to some degree (in this case walking and running).
Ideally we want our tendons to be stiff and strong.
Optimal levels of load on the tendon will result in adaptation to strengthen the tendon and accommodate for the load being applied to it.
However, if the load applied is too excessive or there are sudden changes in load e.g.:
- Running every day and not allowing sufficient recovery from fatigue
- Suddenly increasing running distance too quickly
- Changing running shoes
Then the tendon responds by thickening portions of the affected tendon causing pain.
This is not an inflammatory problem, rather it’s called a reactive tendinopathy.
From this point the reactive tendinopathy can settle with adjustments in load, treatment and exercise which we will discuss later.
However, if the excessive load continues to roll on, the tendon may then reach a point where it begins to breakdown (tendon disrepair) or further to the point it becomes much harder to treat (degenerative tendinopathy).
REASONS FOR DEVELOPING A HAMSTRING TENDINOPATHY
The most common tendinopathy seen in middle to long distance runners is an Achilles tendinopathy.
So what puts the runner at risk of developing a hamstring tendinopathy? Some potential reasons may include:
- Decreased gluteal activation (overloading the hamstring muscle group)
- Decreased hamstring muscle activation
- Longer stride length
- This is issue that seems to come back to the thought that our hamstrings need to be as flexible as possible to minimise injury and improve performance (which is not necessarily the case).
- Having a shorter stride length with good hamstring control during the swing phase will prevent the hamstrings from contracting from a lengthened position and provide a spring effect, which is more energy efficient for running.
MANAGEMENT
Acute
- Rest – At this point, some times it is best to just rest and let that acute flare-up settle down
- Heat – Although this goes against the typical acute injury management acronym RICE, a tendinopathy is not inflammatory in nature. 20 minutes with a heat pack on your buttock/hamstring will be fine
ISOMETRIC EXERCISES
There is evidence to support that isometric resistance training can reduce tendon pain immediately for up to 45 minutes (Rio et al 2015)
Delaying the beginning of an eccentric exercise regime (discussed next) and spending up to 2-3 weeks focusing on isometrics to get the pain under control seems to be working quite well with a number of patients I’ve seen more recently.
- Isometric exercise can be utilised as a form of analgesia
- Start these around day 3 after the initial acute flare
- 5 x 45 seconds at 70% of MVC
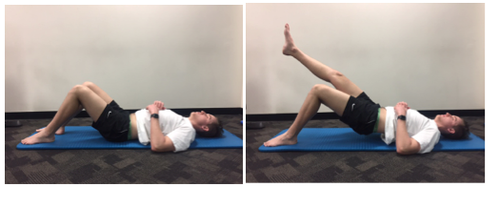
- Lift your unaffected leg off the floor
- Use your affected leg to push down through your foot and lift your bottom up off the floor
- Hold this position for 30-45 seconds if you can
- Generally your buttock / hamstring pain should improve as you continue to perform the isometric exercises
Eccentric strengthening
Eccentric strengthening has been the backbone of tendon rehabilitation for a number of years now. Eccentric exercise has been proven to alter tendon pathology potentially resulting in an improved ability of the tendon to absorb load (Alfredson & Cook, 2007).
Eccentric strengthening exercise involves loading the affected tendon only through the ‘lengthening’ phase of the exercise involved.
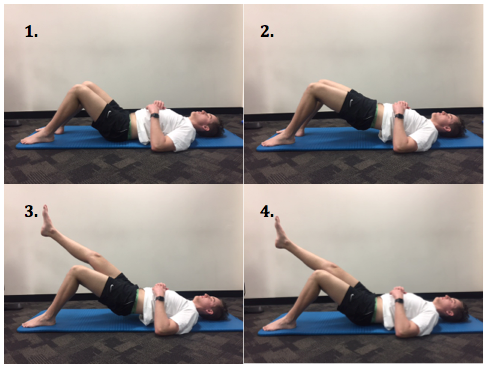
ECCENTRIC BRIDGE
4 sets of 12-15 reps.
- Set your feet and knees shoulder width apart
- Lift your bottom up
- Raise your unaffected leg while keeping your bottom up
- Slowly lower yourself back down controlling with the affected leg
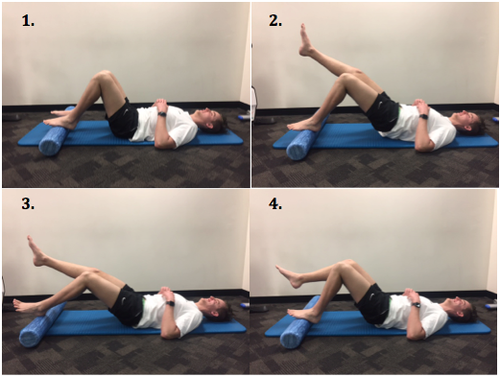
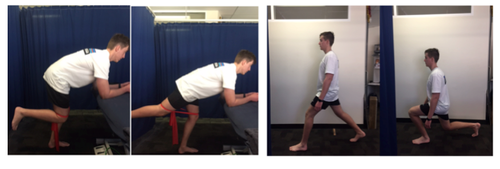
ECCENTRIC BRIDGE WITH ROLLER
4 sets of 12-15 reps with smooth control of hip/knee extension.
- Start with feet and knees shoulder width apart on roller
- Lift bottom up off floor using just your affected leg
- Slowly roll the foam roller away
- Slowly roll the foam roller back to it’s starting position and lower your bottom
Incorporating the full chain
GLUTE ACTIVATION
- The gluteal muscles should be the primary muscle group producing extension at the hip when running. Having under active glute muscles may result in overload of the hamstring muscle group, as the hamstring compensate by acting as a hip extensor.
- These are a couple of exercises that could be included in your rehabilitation program.
HOPPING
I recently attended a great lecture from Mr James Debenham and Dr Merv Travers that discussed the theory of the entire lower limb as a spring, made up of 3 small springs at the ankle, knee and hip.
Ideally we want our spring to be ‘stiff’
Hopping and skipping exercises aim to improve the ease at which our body can leave the ground and continue to propel us forward.
LOAD MANAGEMENT
Managing load is a fine balance between preventing injury and maximising performance. The figure below represents the balance between protein synthesis and protein degradation.
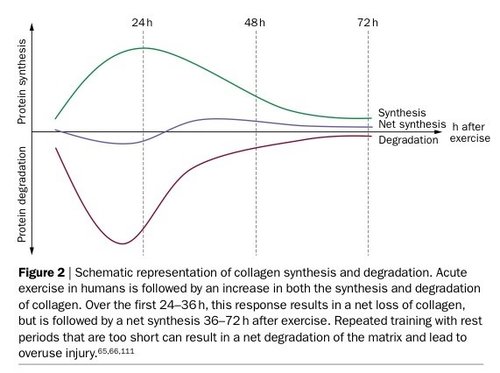
Magnusson et al. (2010)
Based on this diagram we can see that 24 hours after running, the tendon is still at a point of net degradation.
Continuing to run day after day as the body is fatigued will result in ongoing degradation of the tendon.
However, at 48 hours following running the tendon is at a point of net synthesis.
Basically you should be running every second day as this is the point where the tendon is at its safest point for you to continue training and to continue strengthening your tendon.
Ultimately we need to individualise load management based on your level of running, running goals and the point at which you sit on the tendinopathy spectrum.
A FINAL THOUGHT
A question I kept coming back to was why the management of an Achilles tendinopathy was proving more consistent and effective than the management of a proximal hamstring tendinopathy.
One thought I had was that those with an Achilles tendinopathy get a chance to completely unload the Achilles when sitting down.
Those with a hamstring tendinopathy are often constantly reminded of their pain when sitting.
If one of the patients risk factors for the hamstring tendinopathy in the first place was poor gluteal bulk and strength (causing overload of the hamstring tendon during hip extension), this lack of cushioning is likely continuing to aggravate the hamstring tendon as it’s compressed between the ischium and the chair.
Another reason to ensure you continue to strengthen your gluteals as part of your rehabilitation. Maybe having a big bum isn’t such a bad thing!
Sources
- Alfredson H., Cook J. (2007). A treatment algorithm for managing Achilles tendinopathy: new treatment options. British Journal of Sports Medicine, 41(4): 211-216. doi: 10.1136/bjsm.2007.035543
- Cook, JL. & Purdam, CR. (2009). Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine, 43(6). Retrieved from bjsm.bmj.com/content/43/6/409.short
- Magnusson, SP., Langberg, H. & Kjaer, M (2010) The pathogenesis of tendinopathy: balancing the response to loading. Nat Rev Rheumatol, 6(5): 262-8. doi: 10.1038/nrrheum.2010.43.
- Rio, E., Kidgell, D., Purdam, C., Gaida, J., Moseley, GL. & Cook, J (2015) Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. British Journal of Sports Medicine, 49(19): 1277-83. doi: 10.1136/bjsports-2014-094386.