Decreased ankle dorsiflexion range is linked to ankle sprains, Achilles and patella tendinopathy, patellofemoral pain syndrome (PFPS), ACL tears, tibial stress fractures, ITB syndrome and osteoarthritis.
Have you been diagnosed with any of these injuries but never considered the impact of ankle stiffness? Do you treat patients with persistent ankle, knee or hip pain? Is ankle range assessed in all athletes with poor squat control or landing mechanics? What about falls and balance patients?
Don’t forget that ankle range matters!
Why is dorsiflexion range so important?
Walking normally on level surfaces requires about 10° of dorsiflexion (ankle movement bringing the toes up towards the shin bones) and allows people to go up and down stairs, however running and sprinting requires between 20-30 degrees.
Several studies have examined the effects of limited ankle mobility with functional tasks such as double leg squatting, and descending stairs (single leg squatting).
The tasks showed that limiting dorsiflexion range increased the dynamic knee valgus (medial knee displacement causing the leg to roll in), displayed excessive hip adduction and internal rotation, decreased quadriceps activation and increased the soleus (calf) workload.
If you want to improve lower limb control and build quadriceps strength, don’t overlook limited ankle mobility!
Clinical evidence
A recent systematic review concluded that restricted dorsiflexion range of motion might alter lower limb landing mechanics, which predisposes athletes to injury.
The authors hypothesise that the compensatory change in movement may predispose the ankle and other related joints to injury in both acute and chronic cases.
Another study looked at walking gait in patients with ankle arthritis and limited ankle range of motion.
The affected participants displayed decreased walking speeds, decreased cadence, decreased stride length, and increased stance duration compared to the normal control group.
These studies highlight that a stiff ankle not only changes the way people run, jump, land and squat, but also affect the way people walk.
What causes this reduced ankle range?
A recent ankle sprain (rolled ankle) is the most common cause of ankle stiffness experienced in athletes and the general community.
Although many sprains are considered minor injuries, they can progress to chronic ankle instability if severe or without appropriate rehabilitation.
Persistent symptoms can lead to impingement, osteoarthritis and a reduced quality of life with impaired balance in both young and older populations.
Conditions such as ankle sprains, ankle ligament reconstruction, chronic instability, and even the application of an ankle brace are associated with reduced dorsiflexion range.
It is important to maximize the available range of motion after an ankle sprain to limit future ankle dysfunction, improve performance in sport and reduce falls particularly in the elderly.
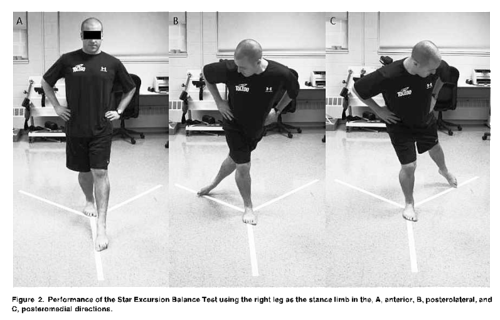
Photo source: Gribble et al. (2012), p. 341.
What about balance?
Dynamic balance measured using the star excursion balance test has been linked to reduced dorsiflexion range in those with chronic ankle instability.
The test shows decreased lower limb balance and control in several directions as well as a reduced ability to step forwards in patients with ankle stiffness.
Range is traditionally measured with a weight bearing dorsiflexion (knee to wall) lunge test and easily reproduced at home to monitor progress in patients.
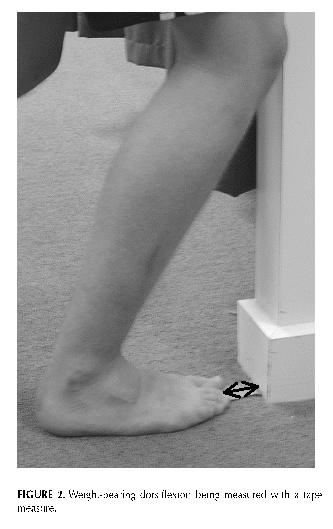
Photo source: Vincenzino et al. (2006), p. 467.
Summary
Injury or trauma to an ankle such as a sprain or impingement problem can limit dorsiflexion range of motion.
This lack of mobility is linked with multiple ankle and knee conditions including ACL injury, stress fractures and osteoarthritis.
From a functional point of view, the lack of range can alter one’s ability to balance, squat, run, land and simply walk, posing a risk of falls in the elderly and increased risk of future injury in athletes.
The authors of a recent systematic review suggest that screening athletes for ankle flexibility may assist in identifying those at risk of further injury, and directing treatment towards modifying this important risk factor.
If you have any ankle, shin or knee complaints, reduced squat depth, poor single leg control or impaired balance, ankle flexibility should always be examined as part of a thorough physiotherapy and biomechanical assessment.
Daniel is team physiotherapist for the Claremont Football Club and is available for biomechanical assessments and screening. He can provide an individualized treatment program to reduce your risk of injury and improve athletic performance.
To book an appointment call (08) 9384 3269 or book an appointment online.
References
Bell-Jenje, T., Olivier, B., Wood, W., Rogers, S., Green, A., & McKinon, W. (2016). The association between loss of ankle dorsiflexion range of movement, and hip adduction and internal rotation during a step down test. Manual Therapy, 21, 256-261.doi: http://dx.doi.org/10.1016/j.math.2015.09.010
Gribble, P., Hertel, J., & Plisky, P. (2012). Using the Star Excursion Balance Test to Assess Dynamic Postural-Control Deficits and Outcomes in Lower Extremity Injury: A Literature and Systematic Review. Journal of Athletic Training, 47(3), 339–357. doi: 10.4085/1062-6050-47.3.08
Hoch, M., Staton, G., Medina McKeon, J., Mattacola, C., & McKeon, P. (2012). Dorsiflexion and dynamic postural control deficits are present in those with chronic ankle instability. Journal of Science and Medicine in Sport, 15, 574–579. http://dx.doi.org/10.1016/j.jsams.2012.02.009
Hoch, M., Staton, G., & McKeon, P. (2011). Dorsiflexion range of motion significantly influences dynamic balance. Journal of Science and Medicine in Sport, 14(1), 90–92.
Khazzam, M., Long, T., Marks, R., & Harris, G. (2006). Preoperative gait characterization of patients with ankle arthrosis. Gait & Posture 24, 85-93.
Macrum, E., Bell, D., Boling, M., Lewek, M., & Padua, D. (2012). Effect of limiting ankle dorsiflexion range of motion on lower extremity kinematics and muscle-activation patterns during a squat. Journal of Sport Rehabilitation, 21, 144–150.
Malliaras, P., Cook, J., & Kent, P. (2006). Reduced ankle dorsiflexion range may increase the risk of patellar tendon injury among volleyball players. Journal of Science and Medicine in Sport, 9, 304–309. doi:10.1016/j.jsams.2006.03.015
Mason-Mackay, A. Whatman, C., & Reid, D. (2015). The effect of reduced ankle dorsiflexion on lower extremity mechanics during landing: A systematic review. Journal of Science and Medicine in Sport, http://dx.doi.org/10.1016/j.jsams.2015.06.006
Vincenzino, B., Branjerdporn, M., Teys, P., & Jordan, K. (2006). Initial Changes in Posterior Talar Glide and Dorsiflexion of the Ankle After Mobilization With Movement in Individuals With Recurrent Ankle Sprain. Journal of Orthopaedic & Sports Physical Therapy, 36(6), 464-471. doi:10.2519/jospt. 2006.2265
Youdas, J., McLean, T., Krause, D., & Hollman, J. (2009). Changes in Active Ankle Dorsiflexion Range of Motion After Acute Inversion Ankle Sprain. Journal of Sport Rehabilitation, 18. 358-374.